What do you think about the possibility of radical healthy longevity?
That’s the idea that, thanks to ongoing scientific progress, new medical treatments may become available, relatively soon, that enable people to remain as vibrant and healthy in their 80s, 90s, and beyond, as they were in their 20s and 30s.
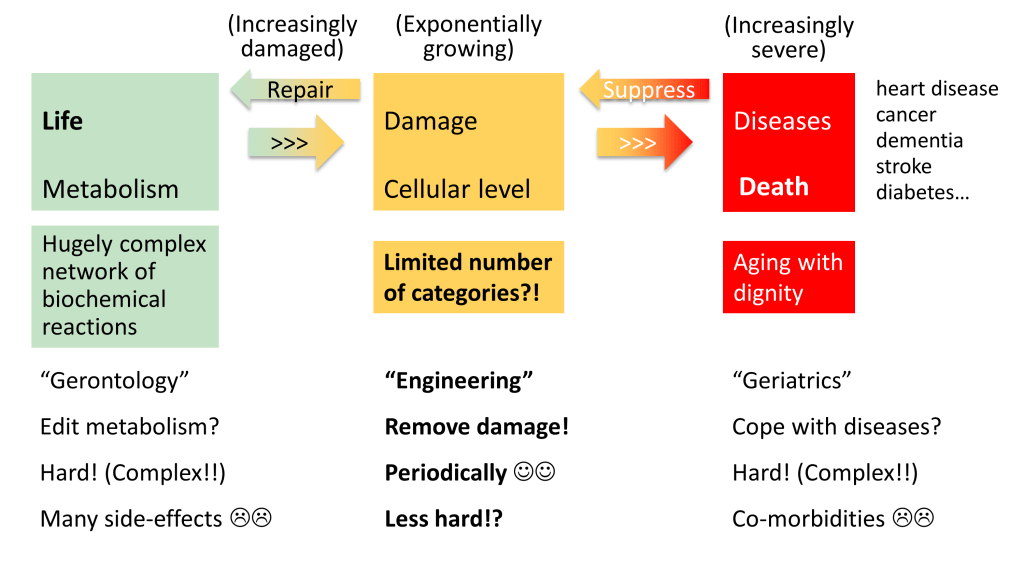
It’s the idea that it may soon become possible to systematically repair or replace, on a regular basis, the various types of damage that tend to accumulate in our bodies over the decades – damage such as plaques, tangles, chronic inflammation, DNA mutations and epimutations, dysfunctional mitochondria, weakened immune function, crosslinks between macromolecules, cells that increasingly neglect their original function, and so on. This damage would be removed before it gives rise to chronic diseases.
It’s the idea, in other words, that aging as we know it – experienced as an inevitable deterioration – could be overcome by scientific innovations, well within the lifetimes of many people who are already adults.
It’s a divisive idea. Some people love it but others seem to hate it. Some people see it as liberating – as enabling lives of abundance. Others see it as being inherently unnatural, unethical, or unjust.
In more detail, I’ve noticed four widespread attitudes regarding this idea:
- It’s an unscientific fantasy. Radical healthy longevity won’t be possible any time soon.
- It will be the ultimate in inequality. Radical healthy longevity will be available only to a small minority of people; everyone else will receive much poorer medical treatment.
- It’s guaranteed that it will be a profound universal benefit. Everyone who is fortunate enough to live long enough to be alive at a threshold point in the future will benefit (if they wish) from low-cost high-quality radical healthy longevity.
- It’s an outcome that needs to be fought for. There’s nothing inevitable about the timing, the cost, the quality, or the availability of radical healthy longevity.
Before reading further, you might like to consider which of these four attitudes best describes you. Are you dismissive, fearful, unreservedly optimistic, or resolved to be proactive?

Who benefits?
To briefly address people inclined to dismiss the idea of radical healthy longevity: I’ve written at length on many occasions about why this idea has strong scientific backing. For example, see my article from May last year, “LEV: Rational Optimism and Breakthrough Initiatives”. Or consider my more recent Mindplex article “Ten ways to help accelerate the end of aging”. I won’t repeat these arguments in this article.
What is on my mind, however, is the question of who will benefit from radical healthy longevity. That’s a question that keeps on being raised.
For example, this is an extract from one comment posted under my Mindplex article:
If you want me to be an anti-aging influencer, the first thing I am going to ask you is “how is this going to be affordable?” How can you guarantee that I not serving only the agenda of the rich and the elite?
And here are some extracts from another comment:
Longevity is ruined by rich people and some elite politicians… Funding for anti-aging research tends to be controlled by those with deep pockets. In reality, the rich and powerful usually set the agenda, and I worry that any breakthroughs will only benefit an elite few rather than the general public… I’ve seen this play out in other areas of medicine and tech (big pharma and cancer are the best examples), where groundbreaking ideas are co-opted to serve market interests, leaving everyday people out in the cold.
The possible responses to these concerns mirror the four attitudes I’ve already listed:
- This discussion is pretty pointless, since relevant treatments won’t exist any time soon. If anything, this whole conversation is a regrettable distraction from spreading real-world health solutions more widely
- The concerns are perceptive, since there’s a long history of two-tier health solutions, compounding what is already a growing “longevity gap”
- The concerns are misplaced, since the costs of profound new health solutions will inevitably fall
- The concerns are a wake-up call, and should motivate all of us to ensure new treatments become widely available as soon as possible.
To restate the fourth response (which is the one I personally favour): we need to choose radical healthy longevity for all. We need to fight for it. We need to take actions to move away from the scenario “the ultimate in inequality” and toward the scenario “a guaranteed profound universal benefit”. That’s because both of these scenarios are credible possible futures. Each extrapolates from trends already in motion.
Extrapolating what we can already see
The scenario “a guaranteed profound universal benefit” takes inspiration from the observation that the cost of products and services often drops dramatically over time. That was the case with computers, smartphones, flat screen TVs, and many other items of consumer electronics. Even when prices remain high, lots of new features become included in the product – as in the case of motor cars. These improvements arise from economies of scale, from competition between different suppliers, and from the creative innovation arising.
But there’s no inevitability here. Monopolies or industry cartels can keep prices high. Strangleholds over IP (intellectual property) can hinder the kind of competition that would otherwise improve consumer experience. Consider the sky-high pricing of many medical procedures in various parts of the world, such as the United States. For example, research by Stacie Dusetzina of the University of North Carolina at Chapel Hill highlights how the costs in the United States of treatment of cancer by the newest pills rose sixfold over a recent 14-year period. That’s after taking account of inflation. And the inflation-adjusted cost of a millilitre of insulin, used in the treatment of diabetes, increased threefold over a recent 11-year period. Many other examples could be listed. In various ways, these examples all fit the well-known pattern that free markets can experience market failures.
A counter-argument is that, provided the benefits of new health treatments are large enough, it will become politically necessary for the state to intervene to correct any such market failures. Early application of the kinds of damage-repair and damage-removal treatments mentioned earlier, will result in a huge “longevity dividend“. The result will be to reduce the costs that would otherwise be incurred as age-related diseases take their toll (often with more than one co-morbidity complicating treatment options). According to the longevity dividend, it’s economically desirable to spend a smaller amount of money, earlier, as a preventive measure, than to have to pay much more money later, trying to alleviate widespread symptoms. No sensible political party could ignore such an imperative. They would surely be voted out of office. Right?
Uncertain politics
Alas, we need to reckon not only with occasional market failures but also with occasional political failures. There’s no guarantee that political leaders will take actions that benefit the country as a whole. They can be driven by quite different motivations.
Indeed, groups can seize power in countries and then hold onto it, whilst giving only lip service to the needs of the voters who originally elected them. Leaders of these groups may assert, beforehand, that voters will prosper in the wake of the revolution that they will bring. But by the way, for the success of this transformation, voters will need to agree that the revolutionary leaders can ride roughshod over normal democratic norms. These leaders will be above the law – 21st century absolute monarchs, in effect. But then, guess what, inflation remains high, unemployment surges, the environment is despoiled, freedoms are suspended, and protestors who complain about the turn of events are rounded up and imprisoned. Worse, due to the resulting crisis, future elections may be cancelled. As for universal access to radical healthy longevity, forget it! The voters who put the revolutionaries in power are now dispensable.
That’s only one way in which the scenario “the ultimate in inequality” could unfold. Less extreme versions are possible too.
It’s a future that we should all seek to prevent.
Choosing to be proactive
Is the answer, therefore, to urge a cessation of research into treatments that could bring about radical healthy longevity? Is the answer to allow our fears of inequality to block the potential for dramatic health improvements?
I disagree. Strongly. On the contrary, the answer is to advance several initiatives in parallel:
- To increase the amount of public funding that supports research into such treatments
- To avoid political conditions in which market failures grow more likely and more severe
- To avoid social conditions in which political failures grow more likely and more treacherous
All three of these tasks are challenging. But all three of them make good sense. They’re all needed. Omit any one of these tasks and it becomes more probable that the future will turn out badly.
As it happens, all three tasks are choices to be proactive – choices to prevent problems early, rather than experiencing much greater pain if the problems are allowed to grow:
- Problems from an accumulation of biological damage inside and between our cells, causing an escalation of ill-health
- Problems from an accumulation of political damage, causing an escalation of economic dysfunction
- Problems from an accumulation of societal damage, causing an escalation of political dysfunction
So, again I say, it is imperative that, rather than passively observing developments from the sidelines, we actively choose radical healthy longevity. That’s biological health, political health, and societal health.

Whether through advocacy, funding, research, or policy engagement, everyone has a role to play in shaping a profoundly positive future. By our actions, coordinated wisely, we can make a real difference to how quickly people around the world can be freed from the scourge of the downward spiral of aging-related ill-health, and can enjoy all-round flourishing as never before.